Sciatica
The role of Physiotherapy in Sciatica management
SCIATICA
Sciatica, Trapped Nerve, Bulging disc, Slipped Disc are conditions frequently treated with physiotherapy. About 10% require a surgical intervention. Sciatica (aka lumbar radiculopathy) describes the symptoms of nerve pain radiating into the leg. It can extend from the lumbar spine into the leg or can sometimes be felt exclusively in the leg without any apparent spinal connection (although it’s actually the source of the problem!).
There is an important clinical difference between nerve pain in the leg as a result of compression in the spine (classic sciatica or lumbar radiculopathy) and referred pain to the leg which can originate from many different structures in the back, pelvis or hip area and is not related to nerve compression.
Clinically this is a very important differentiation and a common error in self-diagnosis.
C
Sciatica is named after the sciatic nerve which is the main nerve running down the back of the leg. The nerve originates predominantlyfrom roots in the lowest 2 joints of the lumbar spine L4/5 and L5/ S1. These are the commonest Lumbar joints to cause problems and as a result the sciatic nerve can become irritated. There is also a nerve that run down the front of the leg (known as the Femoral nerve) and this originates in the upper part of the lumbar spine L1/2, & L2/3. These areas are less common causes of low back pain and therefore the femoral nerve is not frequently involved in leg pain – although it is often referred to as sciatica when present (but technically it’s femoral nerve irritation).

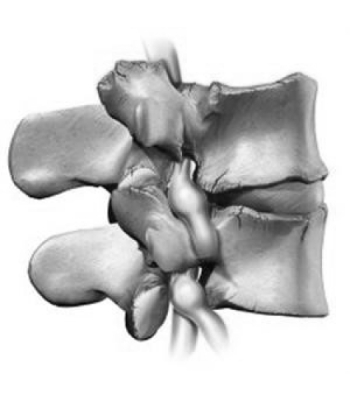
Effects of nerve compression
Like many health issues there is a scale of severity from mild at one end to severe at the other and the type of symptoms which you experience help to define where you are on that scale.
For Appointments, Queries and Expert Advice, Contact us using the button below!
Typical nerve symptoms include the following:
- pain radiating along the line of the nerve ( sciatic nerve)
- sharp, stabbing pain
- shooting, piercing pain
- pins and needles
- numbness
- heaviness
- throbbing
- deep, boring ache
When the nerve is strongly compressed there are additional symptoms such as:
Loss of sensation
Loss of power
Frequently no particular increase in pain which can be deceptive or even missed – but a very important finding!
For Appointments, Queries and Expert Advice, Contact us using the button below!
Causes
About 90% of sciatica is due to spinal disc herniation pressing on the lumbar or sacral nerve roots. Spinal disc herniation, disc prolapse, bulging discs, slipped -disc are all common terms for lumbar disc pathology causing compression of the sciatic nerve. There are many reasons why lumbar discs bulge and will be discussed in a separate article. It is important to recognise that only a small proportion of cases of disc herniation with sciatic symptoms require surgical decompression (Lumbar discectomy).
The statistics for prevalence of sciatica in the general population are quite variable. 80% of the adult population are expected to experience back pain at some point in their life. 30% of those patients will have recurrent episodes of back pain. Estimates suggest that 30% of these patients will have sciatic pain. Less than 10% of cases with sciatic pain require surgical solution which means that 90% are managed in conservatively primary care. Progressive physiotherapy, working on treating causes as well as symptoms is a key part of effective management.
What’s so special about sciatic nerve pain?
There are a number of things about nerve pain that make it different from joint, tendon or muscle pain. Firstly, the intensity of pain is usually more severe. If you have ever experienced sciatic pain (other similar comparable pains would be toothache and shingles) then you will know the feeling.
Secondly, when a nerve becomes sensitive it can become difficult to settle down – even in some cases when the original cause of irritation has resolved. A small proportion of patients with acute nerve pain can develop chronic nerve pain known as neuropathic pain. These cases are difficult to treat, usually require multi-disciplinary management and must be recognised early in clinical practice.
Thirdly, if effective treatment is delayed not only is the potential for the nerve to remain permanently sensitive (chronic pain) but there can also be permanent loss of power and sensation after the pain has resolved.
For these reasons nerve pain is taken very seriously by responsible clinicians and every effort should be made to ensure a speedy resolution along predictable timescales. Importantly great care should be practised to observe the cases when recovery is not proceeding as planned.

Treatment
Physiotherapy treatment in the initial phases of an acute sciatica is primarily geared towards reducing the pressure on the trapped nerve by combinations of graded manual therapy. It is essential manual therapy in this phase reduces the severity of sciatica. Inappropriate manipulation at this point can make a bad situation worse. Trying to “put the disc back” with vigorous manipulation can be highly detrimental and can lead to catastrophic nerve damage.
Treatment is also focused on reducing the inflammatory response both around the bulging disc and also in the irritated nerve itself.
A careful inventory of individual aggravating and easing factors must be established with specific guidelines which are tailored to your presentation. In nearly all cases it is recommended to remain as active as possible but without provoking the sciatic pain.
Formulating these parameters requires detailed questioning and analysis of your symptoms and their behaviour in order to make accurate recommendations and progress the treatment.
As the severity of symptoms improve the emphasis of treatment can shift from first-aid, palliative measures to restoring range of movement and functional capacity. This is achieved by rehabilitating directions of movement that are most restricted (commonly bending forwards).


As specific, painful movements become the focus of treatment it is imperative that the combination of techniques must be applied in a very structured manner in order to be helpful rather than counter-productive. The duration of this sub-acute phase is quite variable and could be between 2 to 6 weeks.
The next phase of treatment is to target muscle control and movement patterns and to identify the underlying mechanics which have contributed to the sciatica. Again this requires detailed analysis of spinal motion, individual spinal segments elasticity, muscle control in the area (frequently referred to as the “core” but the term has become overused, in my opinion) and functional movement patterns.
A huge number of corrective rehabilitation exercises need to be carefully selected, honed and programed into a customised regime to meet your needs. This should follow a sequentially structured progression in order to improve spinal function. As the choice of potential exercise is so vast it is important to zone in specifically on the correct target to ensure a speedy, cost-effective recovery.
BACK PAIN – SPECIFIC CONDITIONS



JOIN OUR MAILING LIST
EMAIL: